

The link between head, neck and jaw pain
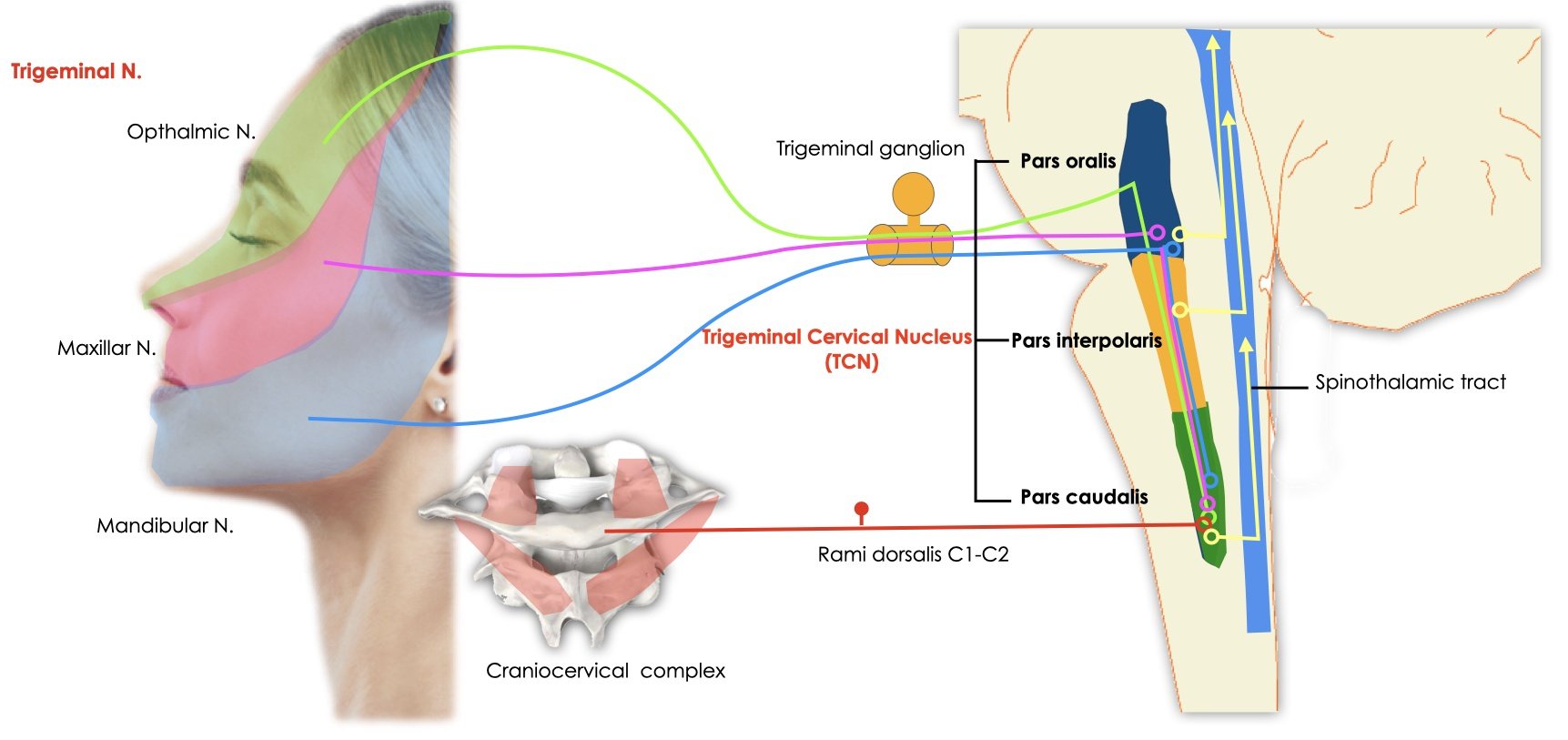
In private practice, a patient’s pain/ dysfunction is typically not isolated to one area. Especially when a patient presents with persistent head, neck or jaw problems, we typically see these areas interconnecting with one another. This cross over in symptoms is now well explained in recent literature. This complex interplay could be simplified to: the face, head and upper neck all share the same nerve supply (trigeminocervical nucleus aka ‘TCN’). As a result the signals sometimes get mixed up and end up being mis interpreted and/or mis directed- like your luggage arriving at the wrong airport!
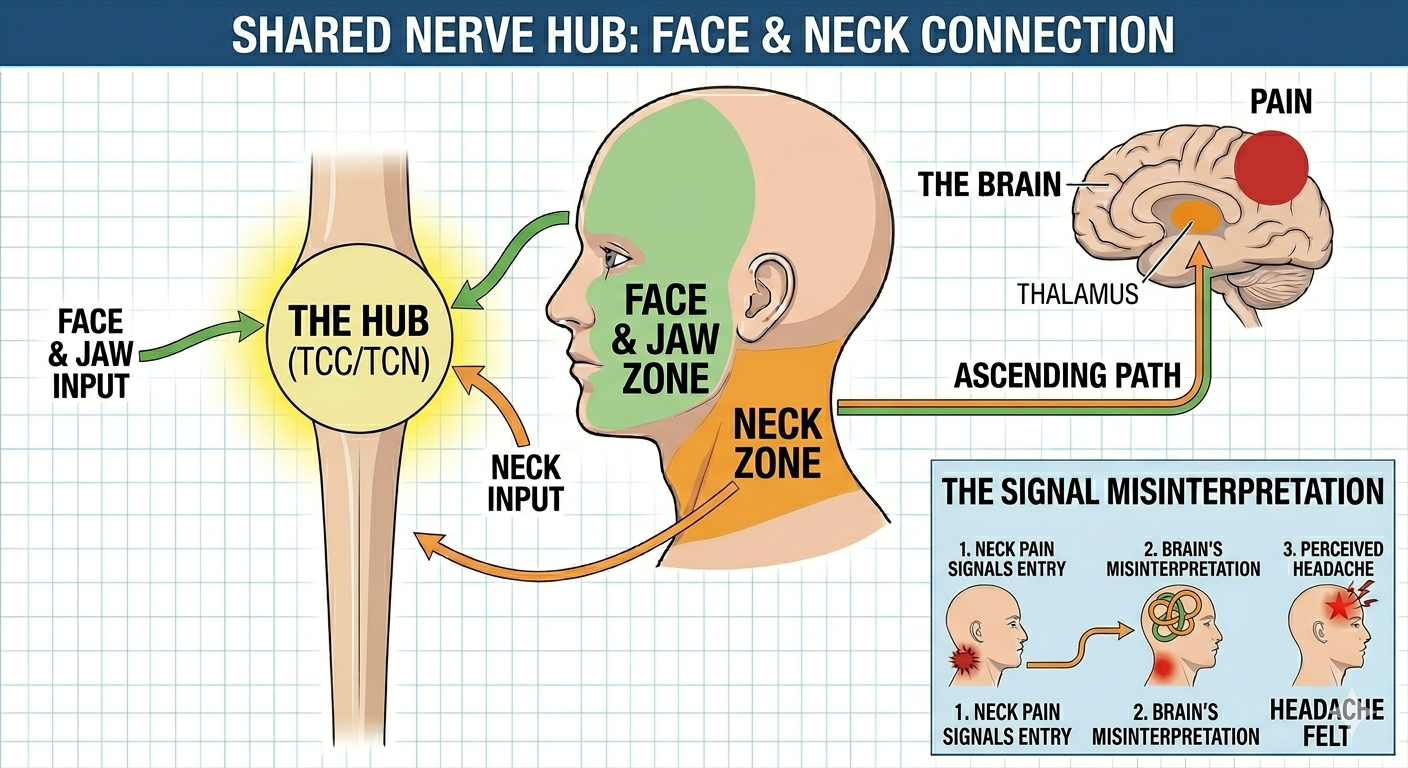
The face, head and upper neck share the same nerve supply?
Let’s think about this with an analogy to airports and major transit hubs like Singapore. For the sake of this analogy let’s say that all pan pacific flights have to transit through Singapore and you have luggage. So if you’re flying from Melbourne to Shanghai, you have a mandatory stopover in Singapore. Also if you’re flying Bangkok to Brisbane, you must stop in Singapore. This means that this ‘transit hub’ is busy with flights coming and going in all different directions. And boarding the wrong flight or your baggage going to the wrong destination is a very real possibility!
This is similar to how the nerves that detect and transmit pain in the head, neck and jaw all share the same ‘transit hub’. They have to ‘stop over’ in the upper neck/ the TCN. And at this stop over, signals can be misdirected and misinterpreted.
A scoping review conducted in 2025 concluded that this head, neck and jaw connection is bidirectional- meaning that neck pain can cause face and jaw pain (Felix P et al., 2025). And that jaw and face pain can cause neck pain. This is important for us in the clinic as we need to ensure that we aren’t looking just at a patient's localised area of pain but rather broadening our lens to look a bit further.
“The connection between the orofacial and cervical regions via the TCN exists and is bidirectional; that is, either stimuli from the neck or the orofacial regions can be integrated at the level of the TCN and provide responses in either region. Therefore, the TCN is a crucial piece in the puzzle of understanding the relationship between these areas. It is strongly recommended clinically that all regions be considered in the evaluation and management of individuals with orofacial, cranial, and/or cervical dysfunction and pain.” (Felix P et al., 2025)
Note. Reprinted from Integration of nociceptive activity from orofacial, cranial and cervical regions in the trigeminocervical nucleus: a scoping review with clinical implications. by Felix P., Pelai, E., Oliveira-Souza, A.,Baghbaninaghadehi, F., Dennett, L., Svensson, P., Piekartz, H., Armijo-Olivo, S. (2025). Journal of Oral & Facial Pain and Headache. https://doi.org/10.22514/jofph.2025.042
,
Broadening our lens on head, neck and jaw pain.
As Osteopaths we appreciate that every patient is individual, so below are just four of the areas we may be addressing in the treatment room:
1. Upper neck instability and the link to tight neck muscles
When a joint in the body is unstable, the surrounding muscles can become tight to provide that joint with more stability. In the case of the neck and jaw, a 2020 paper concluded that: “There is moderate and strong evidence that patients with [jaw pain/ TMD] present lower endurance of extensor neck muscle, global and upper neck hypomobility, worse self-reported neck disability” (de Oliveira-Souza et al., 2020). Hence it is important that we do not just relax the sore and tight muscles but to also address any underlying instability in the surrounding joints.
2. Dysfunctional behaviours in the jaw, neck or head
Jaw clenching (or bruxism) is a common dysfunctional behaviour. Our teeth are only supposed to be contacting <20 mins per day. If we have increased contact time this can impact our jaw, neck and head alignment due to an overactivity of muscles. Other dysfunctional behaviours may include nail or lip biting.
3. Alignment/postural stresses in the neck or jaw
A common posture is a head forward posture with the head slightly tilted into extension. This can put a lot of stress on the upper and lower neck as these muscles are lengthened (a sub optimal position to generate force) and are constantly engaged (increase in fatigue) as the centre of mass has shifted forwards. A low tongue posture can further contribute to this forward head posture, compounding the pressure in the upper and lower neck.
4. Dysfunctional breathing patterns
The diaphragm (a dome shaped muscle located in the middle of the trunk) is supposed to be our main driver for breathing. However due to our modern lifestyle a lot of people have adopted an accessory muscle dominant breathing pattern, using their neck and shoulder muscles to breathe. These muscles can assist but they will be over worked and become tense if they are constantly utilised.
Addressing pain in the head, neck and/or face can seem overwhelming but it is always best to take it one step at a time. First and foremost let’s make you comfortable then let’s have a broader look at what is going on and create a plan to move forwards.
References:
De Oliveira-Souza, A. I. S., de O. Ferro, J. K., Barros, M. M. M. B., & Oliveira, D. A. de. (2020). Cervical musculoskeletal disorders in patients with temporomandibular dysfunction: A systematic review and meta-analysis. Journal of Bodywork and Movement Therapies, 24(4), 84–101. https://doi.org/10.1016/j.jbmt.2020.05.001
Felix P., Pelai, E., Oliveira-Souza, A.,Baghbaninaghadehi, F., Dennett, L., Svensson, P., Piekartz, H., Armijo-Olivo, S. (2025). Integration of nociceptive activity from orofacial, cranial and cervical regions in the trigeminocervical nucleus: a scoping review with clinical implications. Journal of Oral & Facial Pain and Headache. https://doi.org/10.22514/jofph.2025.04